Reading post mortem CT (PMCT)
What generally should be avoided, both on a level of case reading and on a level of providing adequate staffing, is the assumption that reading and documenting PMCT is a matter of a few minutes
Set up the monitor
A monitor or also print output should be set up so grayscale images are rendered adequately1.
The contrast square sequence in the below image demonstrates a number of shallow contrasts that any screen or print quality may be tested or (where adjustable) improved on; every square contains a slightly brighter (A-C) or darker (D-F) square.
For a computer display, the user settings for brightness and contrast as well as lowering the ambient light, usually to around 50-100 lux, may be used to achieve a good visual delineation.
Color references as hexadecimals2.
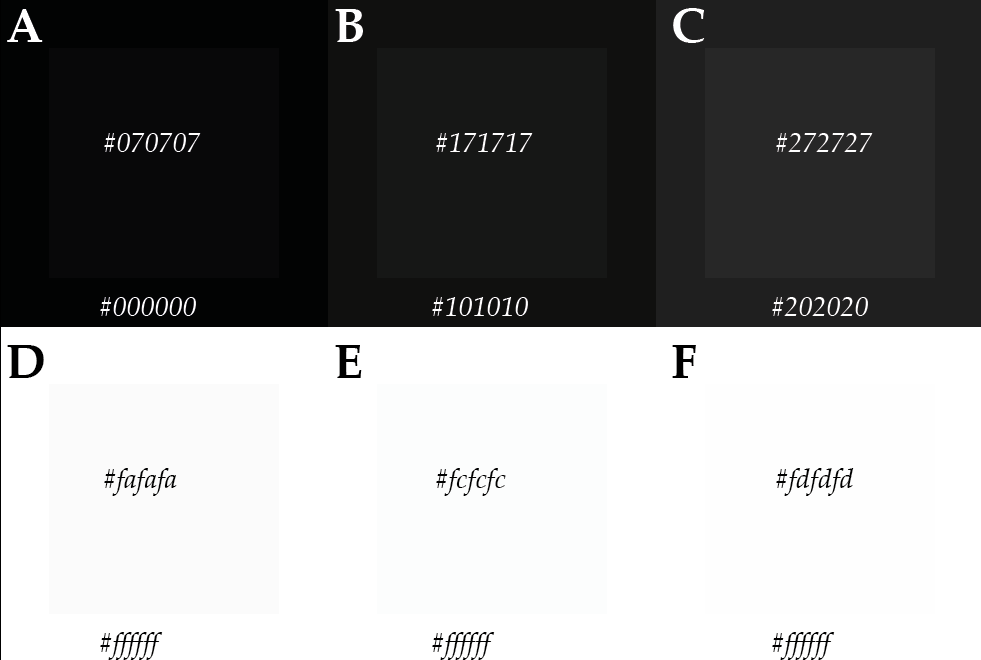
[Image by Wolf Schweitzer, CC BY 4.0]
It is recommended to set up the computer screen to show as much of differentiation of gray levels as possible. To that end, calibration or test patterns can be very useful. There exist a range of purposemade test patterns to help evaluating a monitor or printed product, or, to help calibrating a setup for improvement.
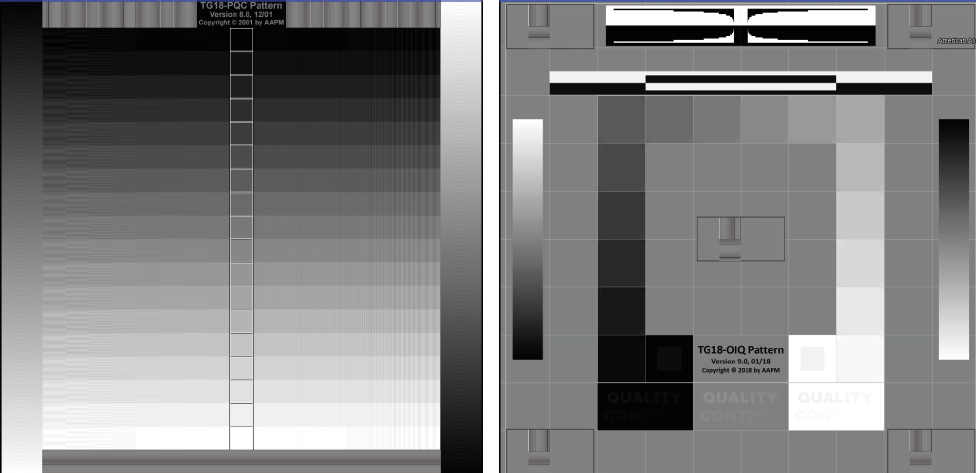
Left: TG18-PQC pattern, Version 8.0, 2021 (C) Copyright 2001 by AAPM. Right: TG18-OIQ Pattern, Version 9.0, 01/18, (C) Copyright 2018 by AAPM. – Cited source: Samei E, Badano A, Chakraborty D, Compton K, Cornelius C, Corrigan K, Flynn MJ, Hemminger B, Hangiandreou N, Johnson J, Moxley M, Pavlicek W, Roehrig H, Rutz L, Shepard J, Uzenoff R, Wang J, Willis C. Assessment of Display Performance for Medical Imaging Systems, Report of the American Association of Physicists in Medicine (AAPM) Task Group 18, Medical Physics Publishing, Madison, WI, AAPM On-Line Report No. 03, April 2005 [use with explicit written permission by Prof Samei under condition that source is cited]
Set up the workspace
The setup for radiology image viewing may be tested using test patterns such as shown above. The computer display and the ambient light should be adapted until all contrast pairs can be seen. In a printed product, these may serve as print quality indicator.
But the computer screen is not the only issue for a proper setup.
Radiological images are read ideally in a room that is not too bright, using computer screens with a sufficient brightness, pixel and contrast resolution. The ambient room brightness, the type of computer display or monitor and its particular setting with regard to brightness, contrast, as well as a possibly more refined calibration, may be regulated by law, regulation or quality requirements3.
Also, the visual acuity of the person reading the images will have to be sufficiently high4. Distraction of any auditory, visual or even olfactory type is to be avoided, as illustrated in the symbolic image below.
Any workflow distraction may be inefficient, in that it extends overall work effort, in one study by a significant extra time cost of up to 13 percent5, as well as increasing the likelihood of an error6.
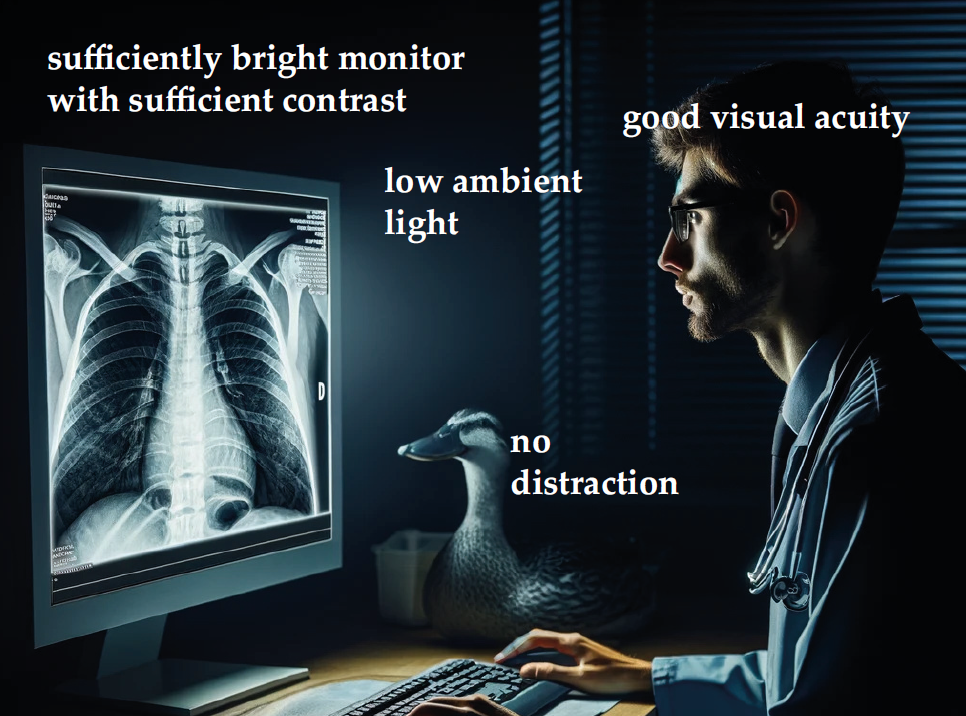
[Image by Chat GPT with a prompt created and submitted by Wolf Schweitzer, CC BY 4.0]
Reading the case
This is a subject for another in-depth review, as much is to be said about technically approaching case reading for forensic PMCT.
What generally should be avoided though, both on a level of case reading and on a level of providing adequate staffing, is the assumption that reading and documenting PMCT is a matter of a few minutes.
A historically early Virtopsy promise was that “CT scanning to document any bone injuries and gross pathologies takes only minutes and can be used as a screening tool”7.
Performing a PMCT scan as such may require anywhere between 10 to 30 minutes, having data exported, transferred or sent to the reading system may take another 5 to 45 minutes, depending on specifics.
Then, a full PMCT reading and documentation should be allowed to take up to, or more than, one and a half to two hours8.
Technically, as a rule of thumb, every body region should be viewed and checked thoroughly several times at least. One should read every body region at least three times in 3D (skin density, bone density, metal density, check from all angles) and four times in axials (focus on soft tissue, focus on bone, focus on gas / air lung densities, focus on metal density) and there, preferrably also in sagittal and coronal view. That means every region is checked a total of seven times using different viewing techniques for a complete coverage. It may be considered to add further techniques, see below.
Report format
This schematic overview symbolically illustrates the extent of visual (V) and written (W) report pages that also I may recommend to consider for routine use. Actual extent, visual and text content details will have to be prepared if not negotiated with the investigators and pathologists.
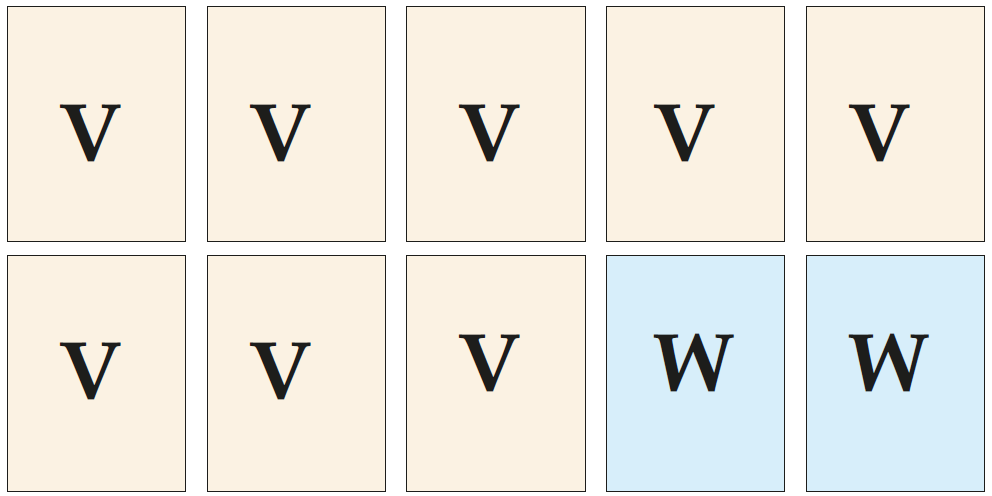
[Image by Wolf Schweitzer, CC BY 4.0]
However, the thought process behind the reporting directly ties into the question of what is relevant in the context of forensic medicine and imaging.
There, stakeholders may have particular expectations.
The employer or head of department wishes PMCT reading to be both done in virtually no time and without missing the smallest findings. They will say “just have a quick look” and “but you did not miss that there was a small osteophyte”. They will say “I just want to get the big picture” whereas we all know the big picture often is pieced together with many small puzzle pieces. They both appear to carry the risk of low quality work and the cost of high quality work.
The pathologist that performs the autopsy or writes the final report about the case when just an external inspection is done but no autopsy is done may prefer the report of the PMCT to be comprehensive. That requires a certain completeness both anatomically and in terms of pathology and trauma or the absence thereof.
The job of attorneys may be to find relevant aspects that were overlooked or overinterpreted or underinterpreted. That requires the PMCT documentation to provide also words, on top of images.
And the relatives, families or friends of the deceased will be interested in the question whether the PMCT has been looked at properly. That usually cannot be communicated convincingly on just one page.
That means that while some forensic pathologists may focus on what they believe to be relevant, neither the state attorney, legal representative of the bereaved or defense lawyer, may share that focus.
So a more comprehensive or wider angle on the subject of reporting may help here. And while one could always write a footnote or disclaimer stating that more data could be analysed, the relevant quote here is “quod not legitur not creditur”, what cannot be read cannot be believed, and “quod non est in actis non est in mundo”, what is not in the files is not in the world.
With that quote – what is not in the files is not in the world – one should approach the reporting of forensic PMCT.
Written report
Reading templates for the written report can be found here, including short guide/indications for the reconstructions or renderings to look at: [english] [german]
From prior materials that I wrote up under CC BY 4.0. Shown across a few presentations but not published previously.

- Samei E, Badano A, Chakraborty D, Compton K, Cornelius C, Corrigan K, et al. Assessment of Display Performance for Medical Imaging Systems, Report of the American Association of Physicists in Medicine (AAPM) Task Group 18. Medical Physics Publishing. 2005 April;.
- Jackson W. Representing RGB Color Values: Using Hexadecimal Data Values. In: Jackson W, editor. Digital Image Compositing Fundamentals. California, United States: Apress; 2015.
- Eidgenössisches Departement des Innern EDI AS Bundesamt für Gesundheit BAG. Anforderungen an medizinische Befundmonitore und die technische Qualitätssicherung. EDI;. Available from: https://www.bag.admin.ch/dam/bag/de/dokumente/ str/str-wegleitungen/technische-qs/wegleitung-qs-bwg.pdf. download.pdf/wegleitung-med-befundmonitore-d.pdf
- Quaghebeur G, Bhattacharya J, Murfitt J. Radiologists and visual acuity. European Radiology. 1997;7:41–43.
- Williams LH, DrewT. Distraction in diagnostic radiology: howis search through volumetric medical images affected by interruptions? Cognitive Research: Principles and Implications. 2017;2:1–11.
- Balint BJ, Steenburg SD, Lin H, Shen C, Steele JL, Gunderman RB. Do telephone call interruptions have an impact on radiology resident diagnostic accuracy? Academic Radiology. 2014;21(12):1623–1628.
- Dirnhofer R, Thali M. Virtopsy after More Than Some 100 Cases: Statement and Perspectives of Forensic Imaging by Using 3D Optical and Combined CT/MRI Whole-Body Scanning. In: The VIRTOPSY APPROACH – 3D Optical and Radiological Scanning and Reconstruction in Forensic Medicine. CRC Press, Boca Raton, Florida; 2009
- Sokolovskaya E, Shinde T, Ruchman RB, Kwak AJ, Lu S, Shariff YK, et al. The effect of faster reporting speed for imaging studies on the number of misses and interpretation errors: a pilot study. Journal of the American College of Radiology. 2015;12(7):683–688.